Thyroid Artery Embolisation (TAE)
-
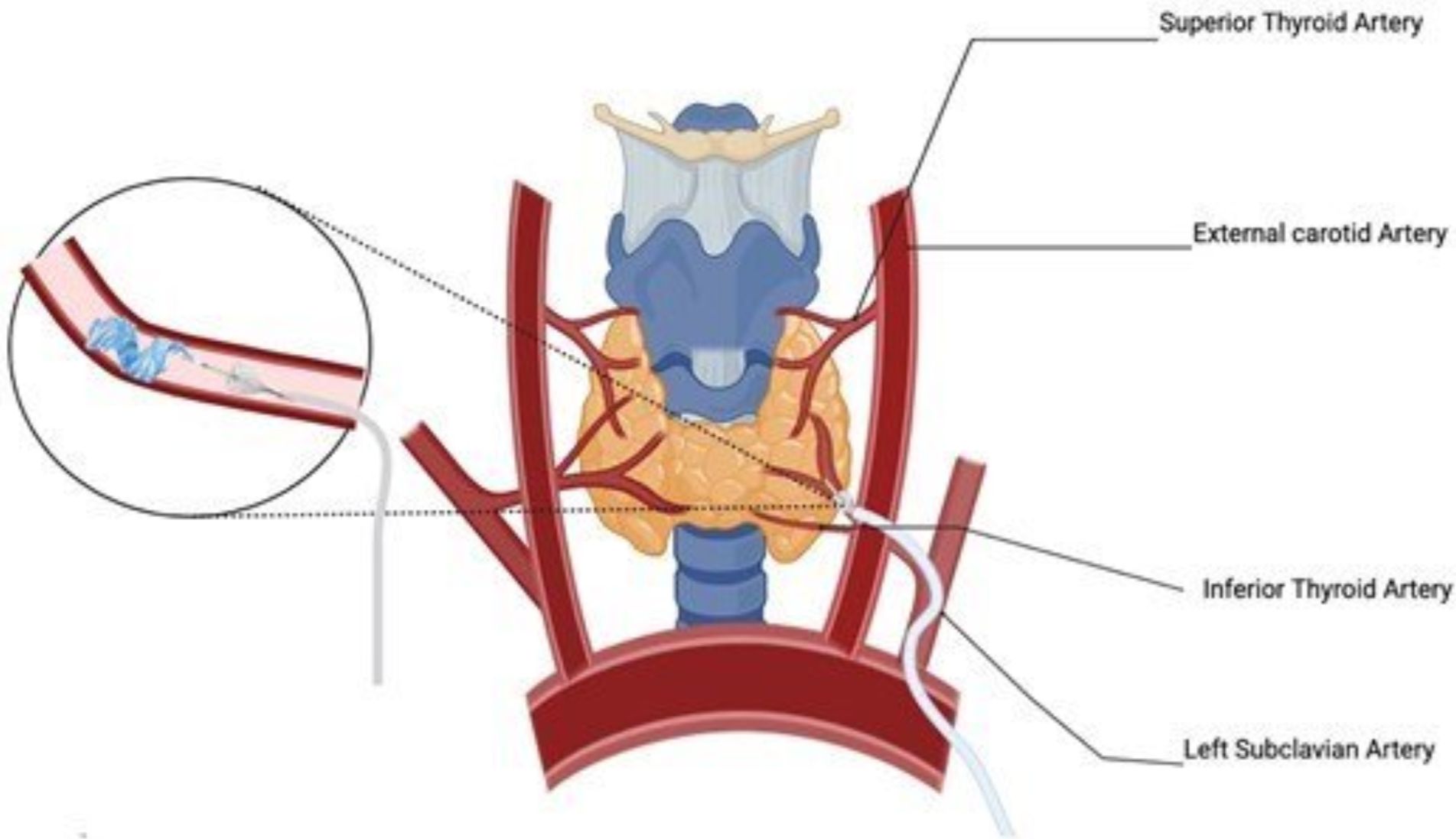
Thyroid Artery Embolisation (TAE) is a minimally invasive, image-guided procedure used to reduce the size and activity of the thyroid gland.
Through a small catheter inserted via the wrist or groin, the arteries supplying the thyroid are selectively targeted. Tiny particles are delivered to reduce blood flow, leading to gradual shrinkage of the gland or nodules over time.
-
TAE provides an alternative to surgery or radioactive iodine for selected patients with thyroid disease.
Advantages
No surgical incision
No stitches
Performed under local anaesthaesia and sedation
Minimally invasive catheter-based procedure
Short recovery time
Suitable for larger or more complex thyroid disease
Can preserve surrounding structures
-
TAE can be used in the management of:
Multinodular goitre (MNG)
Large benign thyroid nodules
Graves’ disease
Patients with compressive symptoms from thyroid enlargement
These conditions may cause:
Neck swelling
Pressure or discomfort
Difficulty swallowing or breathing
Symptoms related to excess thyroid hormone
-
Thyroid artery embolization may be appropriate for:
Patients with symptomatic multinodular goitre(MNG)
Patients with Graves’ disease where other treatments are unsuitable
Patients who are not ideal candidates for surgery
Patients seeking a minimally invasive alternative
Careful clinical and imaging assessment is required to determine suitability.
-
Careful preparation is essential to ensure the procedure is safe, effective, and appropriate for your individual condition.
Prior to treatment, the following will typically be arranged:
Detailed clinical assessment of your thyroid condition and symptoms
Review and optimisation of medications in conjunction with your endocrinologist or treating specialist
Adjustment or temporary cessation of blood thinners where required
Introduction of specific medications for the pre- and post-procedure period (for example to manage thyroid hormone levels and inflammation)
Blood tests, including thyroid function and relevant baseline investigations
A CT scan of the neck arteries to assess vascular anatomy, plan the procedure, and confirm suitability for embolization
-
You will be given instructions regarding fasting prior to the procedure
Most regular medications can be continued unless specifically advised
Arrange for hospital admission
You will receive detailed, individualised instructions prior to your procedure to ensure everything is optimised for a safe and effective outcome.
-
The procedure is performed in an angiography suite under local anaesthesia with sedation.
A small catheter is inserted via the wrist or groin
The thyroid arteries are selectively identified
Embolization particles are delivered in a controlled manner
Blood flow to the thyroid is reduced
The procedure typically takes 1–2 hours. Most patients go home the same day
-
Gradual reduction in thyroid size over weeks to months (up to 50% reduction by 3 months and 80% by 12 months)
Improvement in compressive symptoms
Improvement in thyroid hormone control in selected patients
The degree of response varies depending on the underlying condition and gland size.
-
Thyroid artery embolisation is generally safe when performed by experienced operators. Potential risks include:
Neck discomfort or swelling after the procedure
Temporary changes in thyroid hormone levels
Rarely changes in voice quality
Rare non-target embolization affecting adjacent structures
These risks are minimised through detailed anatomical knowledge and careful technique.
-
Thyroid artery embolization is a technically demanding procedure requiring a detailed understanding of thyroid vascular anatomy.
Dr Bryan Barry is pioneering Thyroid Artery Embolization (TAE) in Sydney and has a focused interest in minimally invasive treatments for complex thyroid disease.
Case study
82 year old female
Large left sided goitre (300 cc) with neck fullness and night time breathlessness
Worsening over last several months
Euthyroid with medical treatment
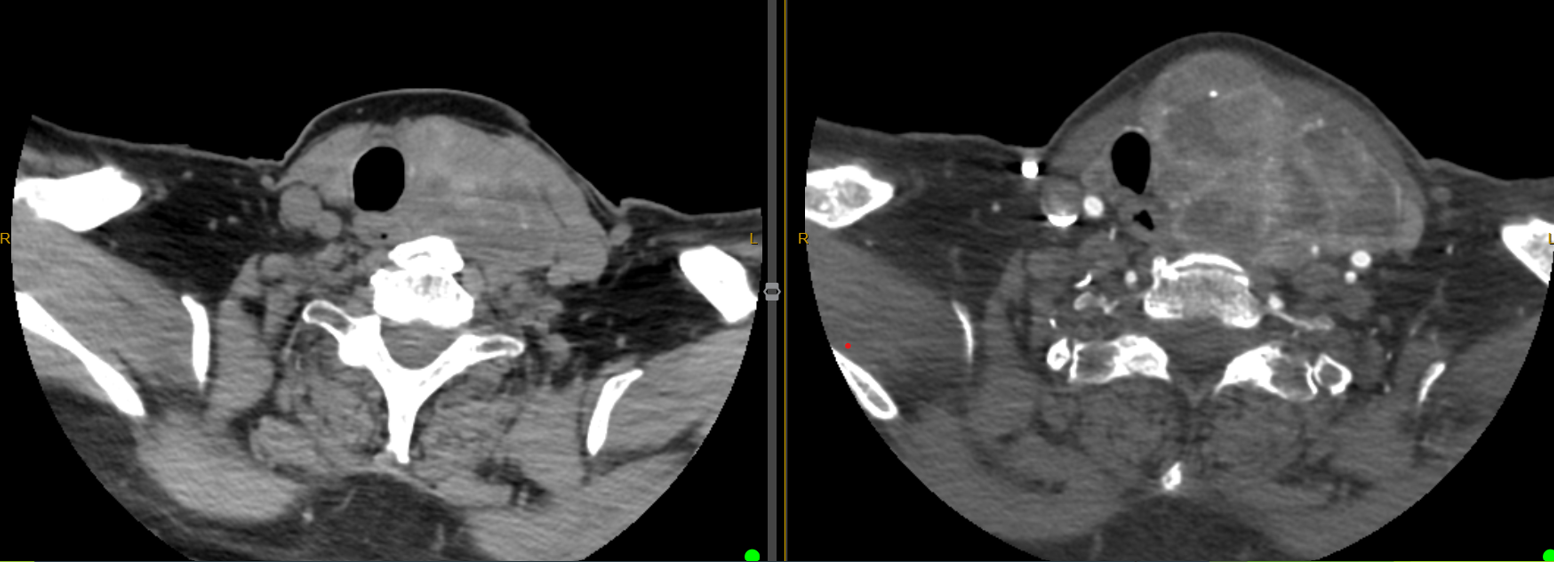
Pre-operative CT demonstrates a 300 cc goitre arising from the left lobe of the thyroid
There is tracheal and oesophageal deviation to the right
Mild tracheal narrowing is observed on the right image
Embolisation was performed as a day procedure
Left image shows marked vascularity and blush on the pre-embolisation angiogram
Right image shows successful devascularisation of the thyroid on the post-embolisation angiogram
Case duration 90 minutes
Discharged home 3 hours post-op
Mild neck discomfort for 1-2 weeks
Symptoms resolved 4 weeks post-op
Euthyroid off treatment after 8 weeks
Left side pre-op CT showing the large goitre with a particularly dominant portion at the left lower pole
Right side post-op CT showing massive volume reduction in the left lower pole component treated by embolisation
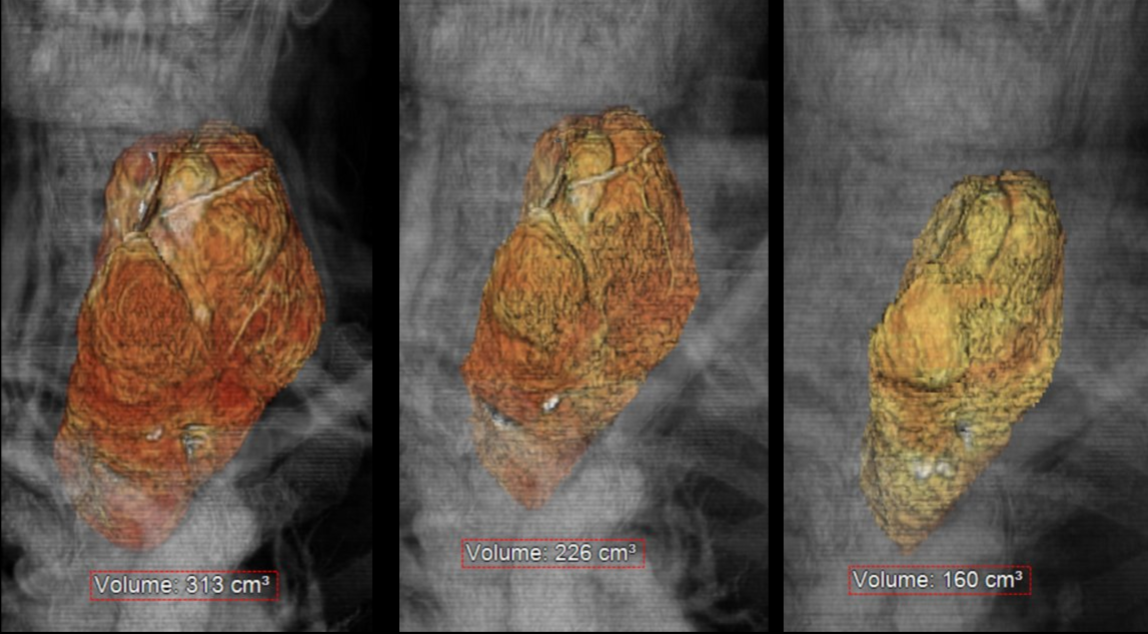
Serial CT scans demonstrate excellent volume reduction of the treatment zone at 1 and 3 months post procedure.