Percutaneous Thyroid Ablation
-
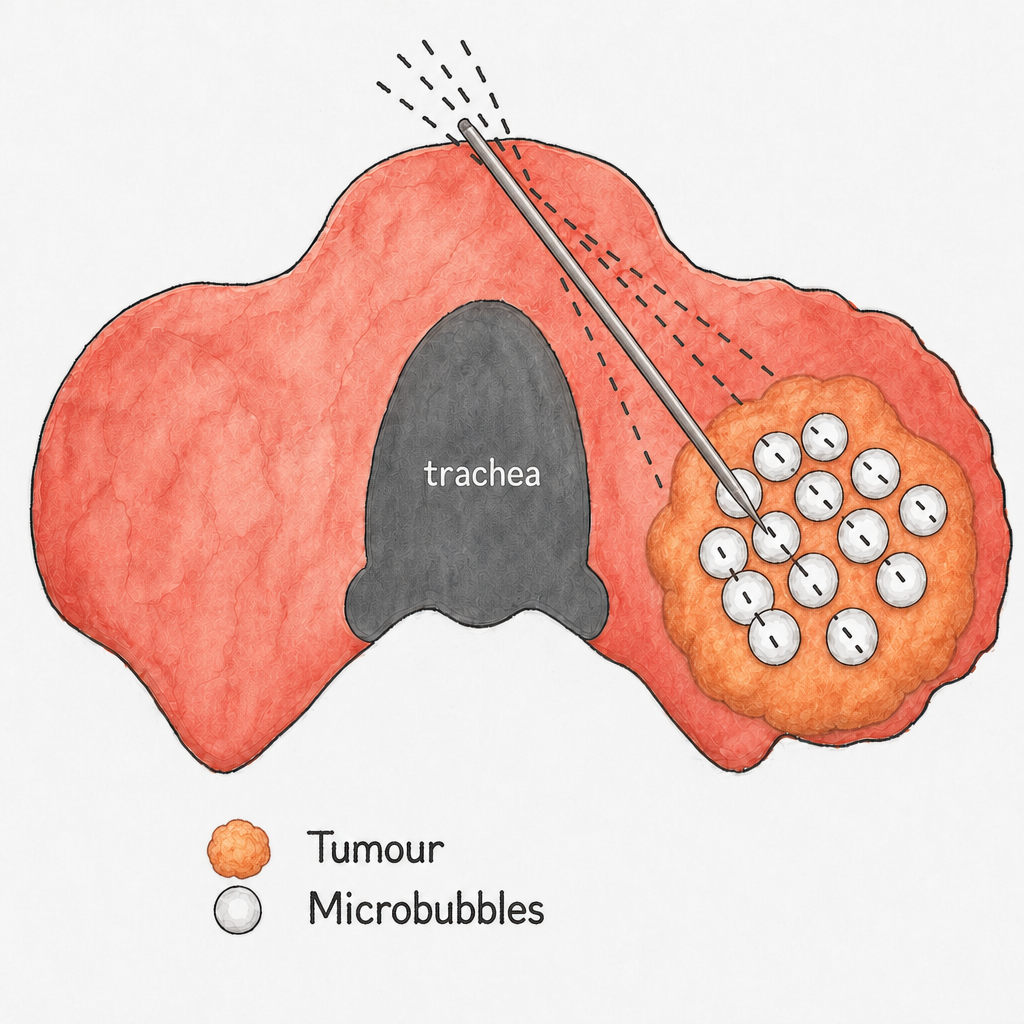
Percutaneous thyroid ablation is a minimally invasive, image-guided treatment used to reduce the size of thyroid nodules without surgery.
Under ultrasound guidance, a fine probe is inserted through the skin into the thyroid nodule.
Controlled energy is applied to selectively treat the nodule tissue, leading to gradual shrinkage over time while preserving surrounding normal thyroid.
-
Percutaneous ablation provides an alternative to surgery for selected patients with symptomatic thyroid nodules.
Advantages
No surgical incision
No stitches
Performed under local anaesthesia (± sedation)
Day procedure in most cases
Short recovery time
Preservation of normal thyroid tissue
Lower overall procedural risk compared to surgery
-
Thyroid nodules are common growths within the thyroid gland. They may be:
Solid
Mixed solid and cystic
Cystic (fluid-filled)
Most nodules are benign and often detected incidentally on imaging.
Some nodules may cause:
A visible lump in the neck
Pressure or discomfort
Difficulty swallowing
Cosmetic concerns
-
Percutaneous thyroid ablation may be appropriate for:
Benign thyroid nodules confirmed on biopsy
Nodules causing symptoms or cosmetic concern
Patients who prefer to avoid surgery
Selected autonomously functioning thyroid nodules (AFTN)
Selected cases of papillary cancer in patients who do not wish to undergo surgery or active surveillance
Careful ultrasound assessment and clinical review are essential to determine suitability.
Dr Barry will work closely with your Endocrinologist or Surgeon to discuss the suitability for percutaneous ablation in a multidisciplinary setting.
-
Prior to treatment, a number of steps are required to ensure the procedure is safe and appropriate. These can be performed in collaboration with your thyroid specialist(endocrinologist or surgeon)
Confirmation that the nodule is benign (usually with minimum of 1 biopsy)
Recent thyroid ultrasound assessment
Review of thyroid function blood tests
Medication review (particularly blood thinners)
Discussion of expectations, outcomes, and potential risks
Fasting instructions if sedation is planned
You will receive specific instructions prior to your procedure.
-
The procedure is performed under ultrasound guidance, typically with local anaesthesia and light sedation.
A fine probe is inserted into the nodule
Energy is applied in a controlled manner
For purely cystic nodules, the nodule is aspirated and a portion of the aspirated fluid is replaced with Ethanol which destroys the lining of the cyst preventing recurrence.
The treatment is monitored in real time using ultrasound +-/- CT
The nodule is treated systematically to achieve optimal coverage
The procedure usually takes 30–60 minutes, and patients are discharged the same day.
-
Gradual reduction in nodule size (up to 40% at 3 months and up to 90% volume reduction reported at 36 months)
Improvement in compressive symptoms
Improvement in cosmetic appearance
For selected autonomously functioning nodules reports suggest a volume reduction of up to 80% may be achieved, which can also improve thyroid hormone levels and functioning.
-
Percutaneous thyroid ablation is generally well tolerated. Potential risks include:
Temporary discomfort or swelling
Bruising
Rarely voice hoarseness or change
Incomplete response requiring further treatment
These risks are minimised through careful planning and experienced technique.
-
If you have been diagnosed with a thyroid nodule and would like to avoid surgery, percutaneous thyroid ablation offers a minimally invasive alternative for selected patients.
We are happy to assess your case and help you understand whether this treatment is suitable for you.
Case Study
35 year old female, prone to scarring.
Focal 33 mm anterior nodule with a volume of 9 cc.
Wanting to avoid surgery and possibility of post-op scarring.
Thyroid ablation was performed using RFA.
The procedure was completed under local anaesthesia, and took 40 minutes to perform.
Patient discharged home 30 minutes post-op.
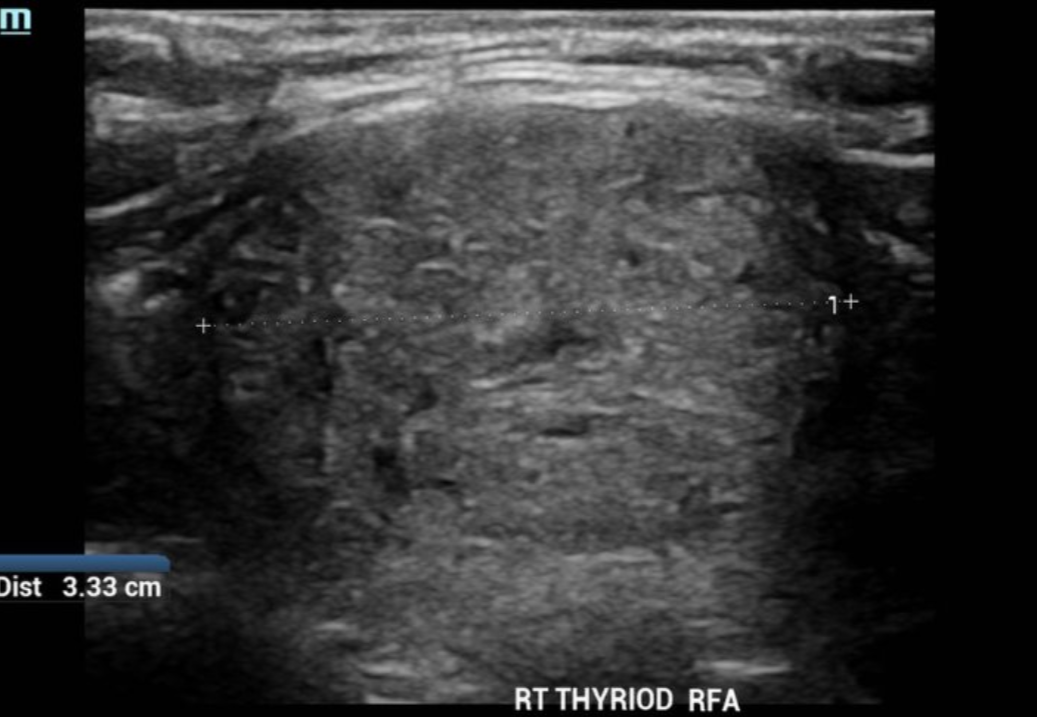

Pre-procedural ultrasound
Nodule measures 33 × 25 × 22 mm
Volume 9 cc
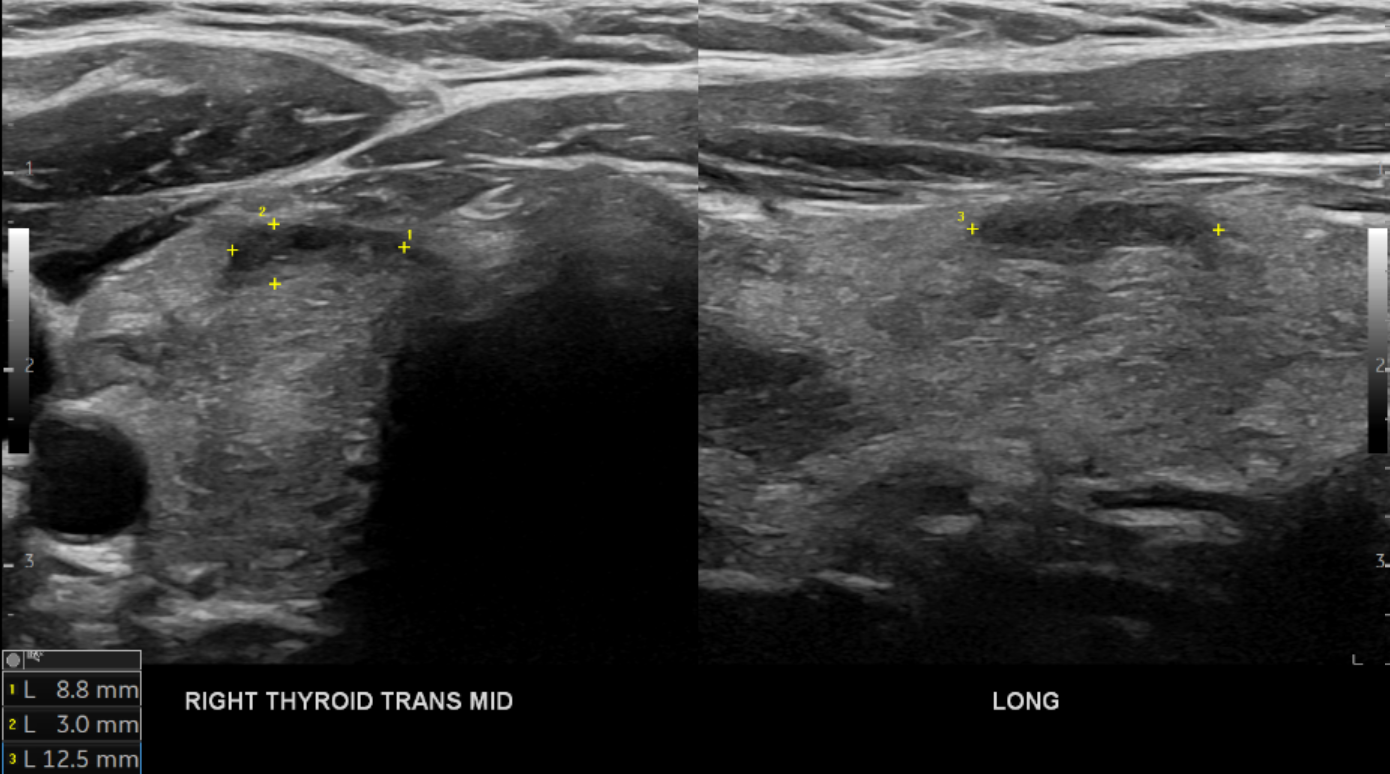
Post-procedural ultrasound after 12 months
Nodule measures 13 × 9 × 3 mm
Volume 0.2 cc
Total volume reduction 98%